
, by NCI Staff

Through ACCURE, health care professionals were trained to understand and respond to the struggles Black people with cancer often face.
Credit: Illustration by Storyset, https://storyset.com/
Although there have been significant improvements in cancer treatment and prevention through the years, a stark reality remains: In many communities, Black people with cancer don’t live as long as White people with the disease.
A collaborative group is tackling this problem head on, making system-wide changes in how cancer centers manage patient care to directly address some of the key drivers of this disparity. A recent study showed that their approach has the potential to help shrink differences in how long Black and White patients with early-stage lung and breast cancer live.
The potential benefit, the study showed, even goes beyond that, by improving survival for all patients with these two cancers.
Experts largely agree that the biggest reason for the long-standing difference in survival is structural and cultural barriers—such as difficulties affording co-pays on medicines and poor communication about treatment side effects—that make it harder for Black patients to complete their cancer treatment. So, the group created a comprehensive program that proactively identified and addressed structural and cultural barriers for every patient.
The program, called Accountability for Cancer through Undoing Racism and Equity (ACCURE), put “systems in place that act as safety nets to help make sure no patient falls through the cracks, whether they are Black or White,” said one of the study leaders, Matthew Manning, M.D., a radiation oncologist at Cone Health Cancer Center in Greensboro, North Carolina.
The group had previously shown that ACCURE helped Black and White patients complete cancer treatment at equal rates. New data from the study suggest that the approach may narrow differences in 5-year survival rates between Black and White patients with breast or lung cancer.
“Other research projects have addressed what can be changed in vulnerable communities or what health behaviors can be changed by individuals,” said Christina Yongue, M.P.H., a former project manager for ACCURE and a professor at the University of North Carolina Greensboro. The novelty of ACCURE, she said, is that it intentionally addresses the changes cancer centers can make within their own institutions to ameliorate racial disparities.
“It’s a moment of awakening that we can make a difference to improve the quality of care that patients receive,” she said.
Ms. Yongue and Dr. Manning reported the findings at the American Society for Radiation Oncology and American Public Health Association annual meetings on October 25.
A multilevel approach to tackling cancer disparities
ACCURE’s beginnings grew out of the Greensboro Health Disparities Collaborative, a diverse group of leaders from the Greensboro community who conduct research and create programs to make health outcomes more equal by race. In the late 2000s, the organization led focus groups with community members to identify barriers to cancer care and to brainstorm potential solutions.
“ACCURE was an implementation of those solutions,” Dr. Manning said. In addition to experts from the Greensboro Health Disparities Collaborative, the NCI-funded study involved researchers and staff from Cone Health Cancer Center, the Universities of North Carolina at Chapel Hill and Greensboro, the University of Pittsburgh Medical Center, and Sisters Network Greensboro.
The intervention included three main parts to improve the rate of treatment completion. The first was a set of nurse navigators who were trained to understand and respond to the struggles Black patients often face, such as mistrust of the medical establishment, miscommunication with their doctors, limited access to transportation, financial hardships, and difficulties taking time off work. These navigators met face to face with each participant several times during the study.
Second, a program was created to alert these nurse navigators in real time if a patient missed an appointment or didn’t meet an expected treatment milestone (such as surgery within 90 days of their first appointment). A nurse navigator then acted as a patient advocate to see what issues the patient was facing and if they could be resolved with available resources, such as free transportation to and from appointments; telehealth visits; rescheduling appointments; advice on pain management; or financial assistance for utilities, rent, or gas.
And third, to enhance accountability, clinical teams were updated monthly on the rates of treatment completion among Black and White patients. That’s a shift from the cancer centers’ standard practice of viewing outcomes individually or independent of race, Ms. Yongue explained.
Many studies focus on single barriers to care, “but this was a multilevel intervention study that explored patient and provider factors in real time in order to make the necessary adjustments,” said Veronica Chollette, R.N., of NCI’s Health Systems and Interventions Research Branch, who oversaw ACCURE’s funding and progress.
Improving survival for everybody with cancer, regardless of race
The new analysis included more than 1,400 people who had been diagnosed with early-stage breast or lung cancer between 2013 and 2015 at a Cone Health facility, and who participated in ACCURE. For comparison, the researchers looked at the outcomes of about 2,000 patients with early-stage breast or lung cancer who had been treated between 2007 and 2011 and who did not participate in ACCURE.
To see if the intervention helped Black patients live as long as White patients, the team looked at the percentage of patients who were still alive 5 years after their diagnosis.
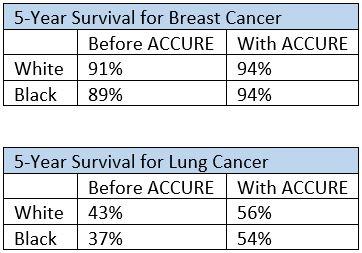
Before ACCURE was introduced, there were small differences in the
5-year survival rates between Black and White people with lung and breast cancer (2% for breast cancer and 6% for lung cancer). With the implementation of ACCURE, survival rates increased for both Black and White people. In addition, the small gaps in survival rates between Black and White patients seemed to shrink (to 0% for breast cancer and 2% for lung cancer).
The study groups were not big enough to show a statistically significant difference in survival rates between Black in White patients before ACCURE, Dr. Manning noted.
But given that the survival rates for Black patients substantially improved with ACCURE, the team believes the intervention has the potential to resolve survival disparities. A larger study would be needed to confirm that, Dr. Manning added.
Addressing barriers to cancer treatment
Most cancer centers have resources to help patients, such as taxi vouchers and assistance paying bills, Dr. Manning explained. But the centers often don’t know which patients need these resources until they’ve already fallen off track.
“What ACCURE did was make it standard operating procedure to identify what those barriers are for everyone. That way we didn’t have to be reactive—we could be proactive,” he said.
The old way of doing things also put the blame on the patient, Ms. Yongue said. Those who frequently missed appointments or didn’t complete treatment used to be called “noncompliant patients,” Dr. Manning added.
“If we can look at it at the institutional level, rather than blaming individual patients, then it changes the conversation,” he said. “I think ACCURE helped to show us that that can be successful.”
Beyond cancer, the team is confident that this sort of approach could help resolve long-standing racial disparities in other areas of medicine, such as diabetes, hypertension, and pregnancy and childbirth complications.
Ms. Chollette agreed. The approach “could be modified to local needs and tailored to address health disparities observed with other cancers,” she said.
For example, she continued, “rural populations are quite challenged with adherence to care due to structural, geographic, and environmental barriers. I think this model could be applied to rural areas where we are seeing health disparities in cervical cancer including low HPV vaccine uptake.”
The ACCURE model is already being adopted in other parts of the country. The study researchers are currently helping various health institutions and private corporations design similar programs to address disparities in their communities.




")

{kind=link}