
, by NCI Staff

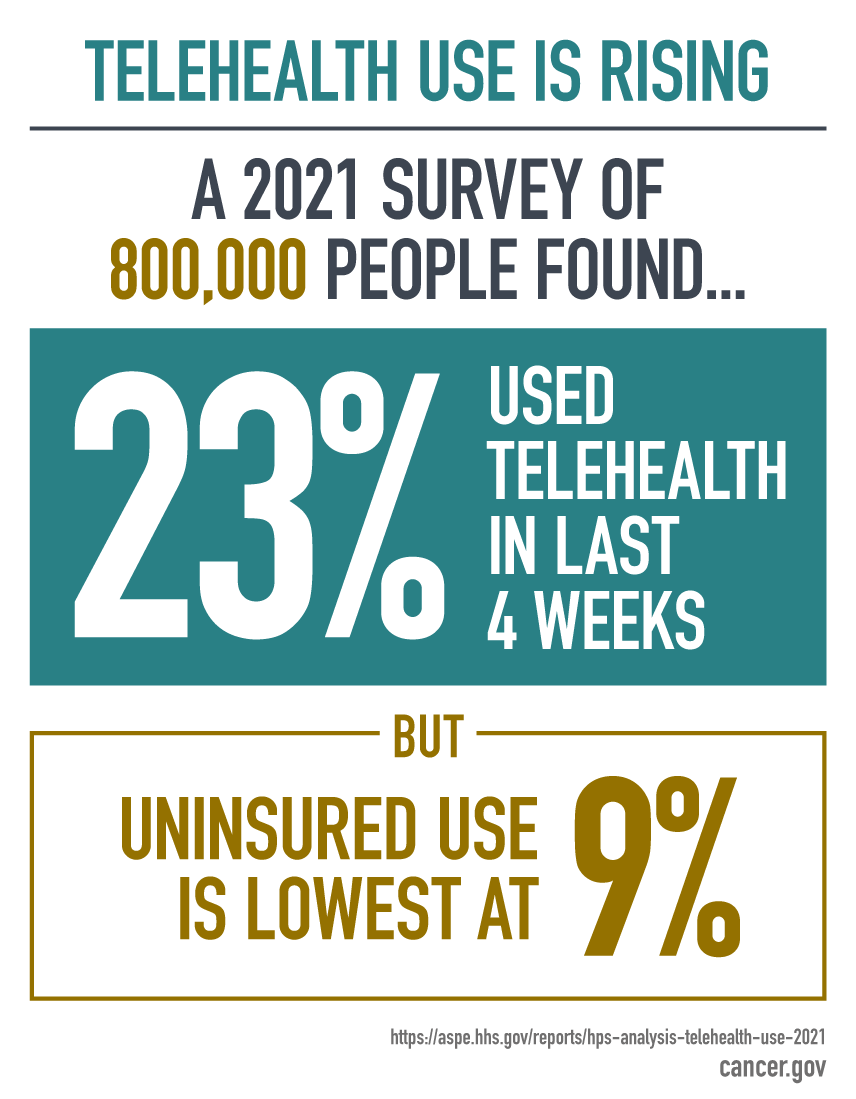
Appointments with health care providers via video and phone calls, known as telehealth, increased dramatically during the COVID pandemic.
Credit: iStock
After their 7-year-old daughter Eva was diagnosed with advanced Wilms tumor in 2020, Chris and Alicia LaBonne sought out a second opinion on Eva’s treatment from doctors at Vanderbilt-Ingram Cancer Center (VICC) in Nashville. But instead of making the two-and-a-half-hour drive from their home in Chattanooga to Nashville for an office visit, the LaBonne family hopped on a video call with a pediatric oncologist at VICC.
“When your child is going through cancer, just those little things—like you get to stay home one more day instead of having to go to the hospital again—can make a big difference,” Alicia said. Doing the visit virtually “just made it so much easier on the whole family.”
During the video call, the VICC oncologist reviewed Eva’s medical records, shared his knowledge of Eva’s specific type of tumor, and discussed treatment options to give her the best possible outcome—all from a laptop set up on the LaBonne family’s kitchen table.
Chris only had to take 30 minutes off from teleworking instead of an entire day traveling to Nashville. That telehealth visit went so well that Chris and Alicia decided to transfer Eva’s care to VICC.
The family then met with a pediatric surgeon to discuss Eva’s surgery plan and a radiation oncologist to coordinate her radiation schedule. Those visits were also done by telehealth. In December 2020, Eva began her treatments in person at VICC.
“If we could have done chemo over telehealth, we would have,” Alicia joked. By July 2021, a scan showed that Eva’s cancer was gone.
For families like the LaBonnes, the option to see health care providers virtually is reshaping their cancer care experience. Although it can’t entirely replace in-person care, telehealth offers patients convenience, time and cost savings, flexible scheduling, access to specialists far away, and what many patients and doctors describe as intangible benefits, such as reduced exposure to germs.
Oncology is not a unique example of telehealth’s growth. From primary care to cardiology, as the use of telehealth surged during the COVID-19 pandemic, so too has the demand for more access to this virtual form of health care.
But experts caution that our understanding of the role of telehealth in cancer care and how to deliver it equitably is still in its infancy. Studies are needed, they say, to help telehealth transition successfully from a temporary solution during the pandemic to a permanent and integral part of the cancer care experience that’s accessible to all who need it.
Virtual cancer care visits catch on
Telehealth, sometimes referred to as telemedicine, is health care provided by doctors and other health care providers from a distance using electronic means. Telehealth visits are typically done by phone or video and can also include email and text message exchanges between a patient and their providers.
In some cases, telehealth may be complemented by remote monitoring of patients, with data on their symptoms being collected electronically using devices such as wearable activity trackers.
The development of telehealth as it’s conducted today can be traced to the 1960s, when NASA developed technology to monitor the health of astronauts while they were in space. Although telehealth eventually found its way into mainstream clinical practice, the COVID-19 pandemic led to its widespread adoption in nearly every aspect of patient care.
Kevin M. Curtis, M.D., medical director of the Center for Telehealth at Dartmouth-Hitchcock Health, said that before the pandemic, this academic medical center was averaging eight scheduled outpatient telehealth visits a day. When the pandemic first peaked in April 2020, the number of telehealth visits swelled to more than 2,600 in a single day.
Although adoption of telehealth at Dartmouth-Hitchcock’s Norris Cotton Cancer Center was initially slower than it was with some other specialties, it has been growing steadily, said Anna Tosteson, Sc.D., of Norris Cotton, who has been studying patterns of telehealth use at the cancer center, along with Dr. Curtis.
“Our experience over the pandemic highlighted the potential for telehealth to be a game-changer with regard to timely access to care,” Dr. Tosteson noted.
“More recently, probably somewhere in the ballpark of about 12% of outpatient oncology visits are done by telehealth,” Dr. Curtis explained, compared with virtually none before the pandemic. The cancer center’s slower adoption of telehealth initially, he added, may have at least partially been caused by limitations in the telehealth platform, which have since been upgraded.
Other NCI-Designated Cancer Centers have also seen a rise in telehealth use during the pandemic. In August 2020, 40% of patient visits at the University of Texas at San Antonio Mays Cancer Center were occurring by telehealth. At the Sidney Kimmel Comprehensive Cancer Center at Jefferson Health in Philadelphia, nearly 7,000 patients were seen via telehealth between March and July 2020, compared with approximately 150 patients during the same period in 2019.
The telehealth surge has been partly aided by temporary policy measures have helped loosen some of the restrictions around telehealth during the public health emergency, such as those preventing health care providers from providing remote care across state lines.
Many states also waived licensure requirements for clinicians to provide telehealth. Now, legislation is working its way through Congress to help make some of these changes permanent. The Telehealth Extension Act, for example, aims to lift geographic restrictions to allow people with Medicare to access telehealth no matter where they live.
Dr. Curtis said it will be important to see what results from some of these legislative efforts, as well as policies around insurance reimbursement and licensure, because those variables could impact hospitals’/doctor’s offices’ willingness to fully invest long term in telehealth. In the meantime, it’s important for the health care community to continue accumulating evidence showing that telehealth provides value to both patients and clinicians, he said.
Telehealth delivers high satisfaction
While these bills move through the legislation labyrinth, many people with cancer have reported high satisfaction with their telehealth visits. According to available data, that appears to be particularly true for certain needs, such as cancer genetic counseling.
Larry Starling’s treatment for male breast cancer at a local hospital is being guided via telehealth by an oncologist at VICC. Contrary to the perception that patients may feel disconnected to their health care providers in a virtual setting, Starling said his telehealth visits have felt more personal than his in-person office visits.
“In an office setting, the doctor is thinking about the next patient,” he said. “Whereas on the telehealth visit, you feel like it’s just you and the doctor and you have their undivided attention.”
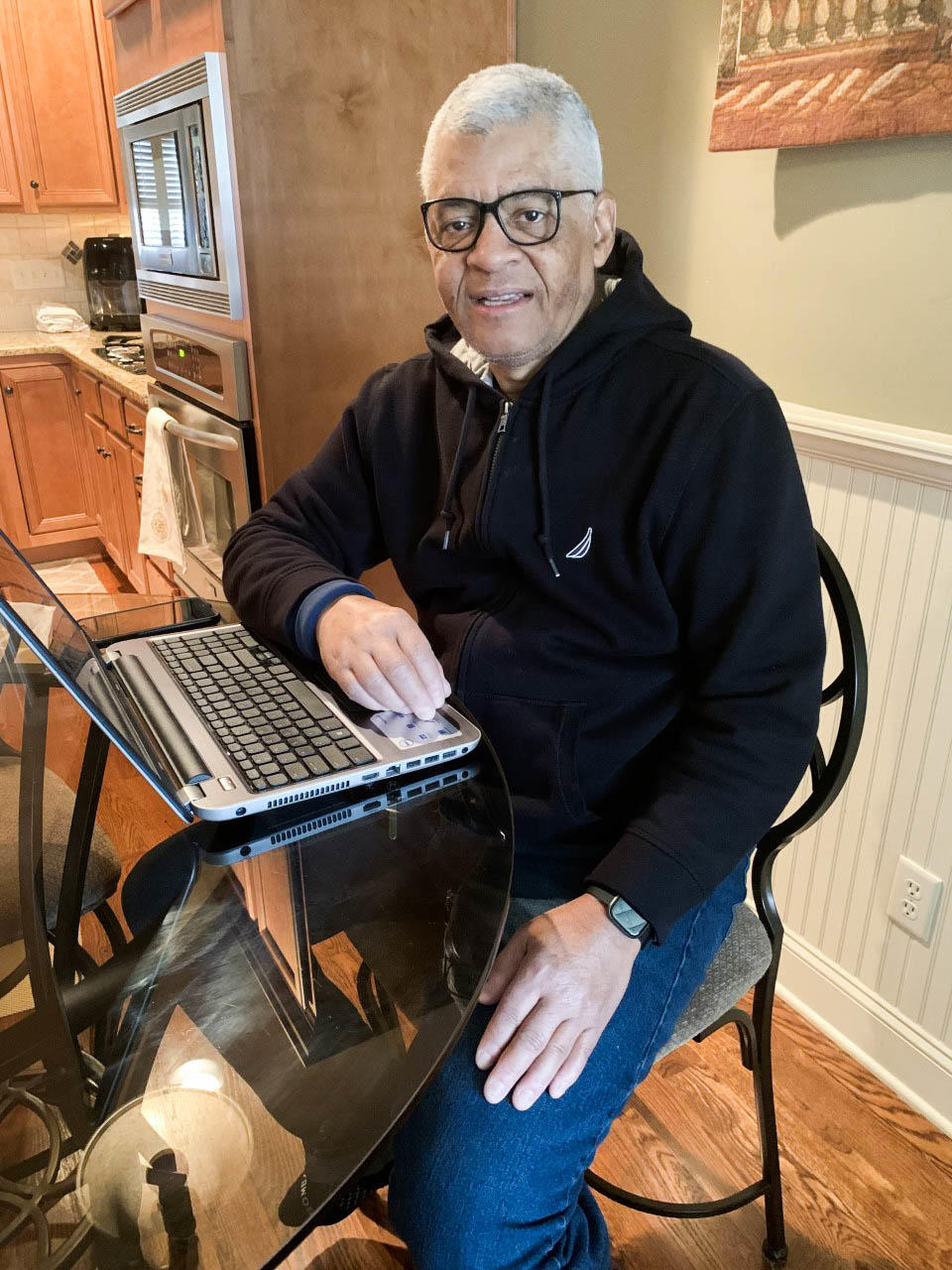
After he was diagnosed with male breast cancer, Larry Starling often met with his oncologist via telehealth.
Credit: Larry Starling
Starling said that his VICC oncologist shares his screen virtually so they can look at his scans together. “The technology is to the point where you almost feel like you’re in the office with him,” he said. “I didn’t lose any feeling of being connected, talking to him over the telehealth visit.”
Clinicians have generally reported high satisfaction with telehealth. In a survey of approximately 200 oncologists conducted in the spring of 2020, the majority were satisfied with telehealth and wanted to continue using it. In fact, nearly 60% of those surveyed believed video visits were sufficient for managing most aspects of patient care, including discussing treatment plans and reviewing laboratory results.
However, the majority felt that in-person visits were preferable for promoting “a strong
physician–patient connection.” In addition, they felt that certain kinds of conversations, such as new diagnoses and end-of-life discussions, were better handled in person.
“There are some things we can’t do via telehealth,” said Debra L. Friedman, M.D., associate director for Community Science and Health Outcomes at VICC, who was not involved in the survey. “There’s no way to do mammography. There’s no way to do a colonoscopy. There’s no way to do a low-dose CT scan for lung cancer screening.”
Addressing health disparities
Amid the increasing demand for telehealth, experts worry that some populations that could potentially benefit the most from telehealth—including older adults and those living in rural areas—may be left behind. Others include people from low-income groups and racial/ethnic minority groups, and those for whom English is not their first language.
“Telehealth has the potential to address disparities. Because marginalized populations can struggle disproportionately with issues like transportation barriers, time away from work, and competing demands for caregiving, telehealth can really ameliorate a lot of those demands,” said Urmimala Sarkar, M.D., associate director of the University of California San Francisco’s Center for Vulnerable Populations.
In practice, though, certain obstacles are preventing telehealth from being a realistic possibility for many people, Dr. Sarkar added. Issues like the lack of high-speed internet, language barriers, and lack of comfort with the technology used to conduct telehealth visits can be insurmountable for many patients.
“What we see is that there’s a difference between that theoretical potential to reduce disparities and the way that telehealth actually functions,” she noted.
“I worry that instead of addressing a disparity, we’re creating a disparity,” said Dr. Friedman. “Because what we [have] found is that the patients who are most likely to use telehealth were the patients who were actually the most served. It was not ethnic and racial minorities, and it was not patients who were of low socioeconomic status. Those struggled with telehealth.”
Researchers at the University of Kansas Cancer Center looked at Medicare claims data from 16,000 people newly diagnosed with cancer to identify patterns of telemedicine use.
Nearly 70% of patients with the highest socioeconomic status had a telemedicine visit within 30 days of their cancer diagnosis, they found, compared with less than half of patients in lower socioeconomic groups. The patients in the highest socioeconomic groups continued to have high rates of telemedicine use in subsequent months, while rates among those in the lowest socioeconomic groups remained low.
Matthew B. Mackwood, M.D., M.P.H., of Dartmouth-Hitchcock Health, who is studying factors influencing telemedicine use among rural populations, pointed out that “the ability to use a telephone is far more universally accessible to individuals” than telehealth visits using video calls.
As the pandemic has slowed down, there have been proposals to cut or restrict health insurance coverage of phone-based telehealth visits. If those changes are made, Dr. Mackwood said, it may exacerbate some of the existing disparities in cancer care.
“In our cancer center, something like 80%‒90% of the telehealth visits are done via telephone rather than video,” he noted.
Dr. Friedman and her colleagues are conducting a clinical trial, called ENCORE, to determine whether supporting doctors and patients in rural hospitals by giving them access to expertise and supportive care from oncologists at VICC via telehealth will enhance cancer care.
She pointed out that doctors currently use a variety of videoconferencing systems, including Zoom, Webex, and platforms integrated into patients’ electronic health records, and that the mix of platforms can be confusing for people who are less comfortable with technology.
“What we’re doing in the ENCORE study is collecting data about what works and doesn’t work,” Dr. Friedman said. “I think we have to have simpler platforms. And I think we’re always going to need some human support.”
From telehealth to teleresearch
Cancer clinical trials have also had to adapt to restrictions imposed by the pandemic.
For example, some aspects of clinical trials are now being performed virtually, particularly for trials that focus on cancer prevention and survivorship, explained Ann Geiger, Ph.D., M.P.H., of the NCI Community Oncology Research Program (NCORP).
Providing patients with information about a clinical trial so they can decide whether they’d like to participate is probably one of the easiest things to do virtually, Dr. Geiger said. Other clinical trial activities that have converted to a virtual setting include completing quality-of-life questionnaires, clinical follow-up visits, pain management consultations, and behavioral treatment for smoking cessation.
One question is whether telehealth will help streamline how clinical trials are conducted, for example by enabling faster patient accrual.
“I don’t think we know the answer yet,” said Dr. Geiger. “It’s such a complicated situation. My hope certainly is that if you reduce the burden on patients—so, instead of having to come in monthly, you’re coming in quarterly—people might be more willing … to be in a trial. But we shall see.”
Looking ahead in telehealth
Beyond telehealth visits by phone and video, another component of telehealth where interest is surging is remote monitoring of patients’ symptoms via mobile phone and other devices.
In a study led by researchers from Huntsman Cancer Institute at the University of Utah, patients used a remote monitoring system to regularly report any cancer- and treatment-related symptoms they were experiencing at home. Patients who do report symptoms get guidance on how to best manage them, including direct follow-up for any symptoms that continue to bother them.
The remote monitoring has been a success. Not only were patients’ symptoms much improved, but they were better able to manage them on their own at home than patients who didn’t undergo remote monitoring.
Future advances in remote monitoring may open up other possibilities as well, such as being able to analyze blood samples at home, said Kathi Mooney, Ph.D., R.N., the study’s lead investigator. “That can be particularly helpful in oncology.”
New technologies, such as artificial intelligence and virtual reality, are also helping to expand the limits of telehealth. An ongoing NCI study, for example, is looking into whether virtual reality technology delivered remotely can help reduce stress and improve mood in adults being treated for brain tumors. Participants view relaxing scenes using virtual reality goggles received in the mail and complete a questionnaire about their symptoms.
Telehealth’s role in cancer care will continue to evolve, Dr. Friedman said. But experts agree that it will involve a hybrid of telehealth and in-person care.
“Telehealth is here to stay,” Dr. Friedman said. “We just have to continue to work on making it more available and simpler for people to use.”
Alicia LaBonne is grateful that telehealth was a part of her daughter’s journey to recovery. “Telehealth is such a big asset right now,” she said. “I hope that it continues for families just like ours.”




")

{kind=link}