
, by Sarah Schmelling

The NIH-led IDENTIFY study is looking at the experience of pregnant people for whom prenatal DNA testing suggests they may have cancer.
Credit: iStock
A blood test that may detect cancer has received some attention recently. But, unlike other blood tests being studied as ways to screen for cancer, it wasn’t designed for that purpose. This test is a prenatal blood test that analyzes free-floating bits of DNA, known as cell-free DNA (cfDNA), from the fetus. Specifically, tests of this type screen for an irregular number of chromosomes, called fetal aneuploidy.
But in the decade or so that noninvasive prenatal blood tests—often called NIPT—have been in clinical use, there have been some cases in which the results indicated that a fetal aneuploidy was present, but additional testing found the fetus had normal chromosomes. In some of these cases, women who received these false-positive prenatal screening results were subsequently diagnosed with cancer, either during the pregnancy or after childbirth.
These reports led NIH researchers to launch a study, called IDENTIFY, in 2019 to learn more about the relationship between these test results and cancer. The study is led by Christina Annunziata, M.D., Ph.D., of NCI’s Center for Cancer Research, and Diana Bianchi, M.D., director of the Eunice Kennedy Shriver National Institute of Child Health and Human Development.
Dr. Bianchi and Amy Turriff, Sc.M., a genetic counselor at the National Human Genome Research Institute, who is also involved in the study, recently talked with Cancer Currents about the experience with the study so far.
Why was the IDENTIFY study launched?
Bianchi: Noninvasive prenatal testing for fetal chromosomal abnormalities first became available in late 2011. In 2013, there began to be reports of inaccurate test results, and occasionally there were confusing results that were interpreted as false positives for fetal aneuploidy. There would be a report that the fetus had trisomy 13 [a chromosomal condition], or that there were multiple aneuploidies, and then the diagnostic testing on the fetus was normal.
Also in 2013, there was a report of a woman who had multiple aneuploidies found in her prenatal test results. Two different labs carried out three tests, all with the same results, suggesting that it was a real finding, but the fetus was normal.
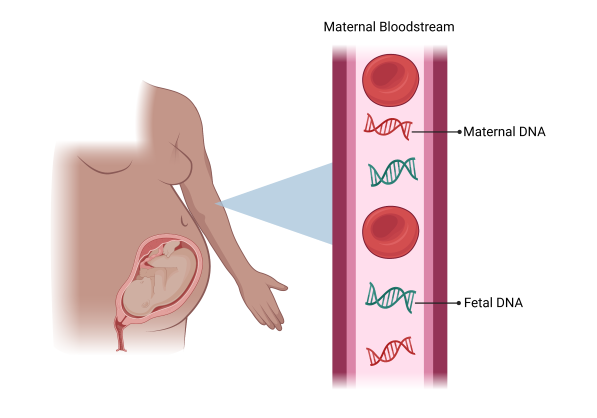
In pregnant people, blood tests that analyze bits of DNA from the fetus to find an abnormal number of chromosomes, or aneuploidy, are routinely performed. In some cases, these tests find aneuploidy in maternal DNA, identifying potential cancers.
Credit: Created with Biorender.com
It was only after the birth of the baby, when the woman complained of pelvic pain and a more extensive workup was done, that she was shown to have pelvic bone fractures that were the result of a neuroendocrine tumor that had spread. The tumor was shedding fragments of DNA into the woman’s bloodstream that were being detected by the prenatal test.
That was the first recognition that tests analyzing cfDNA, supposedly from the fetus, could also detect cancer in the mother.
When I came to NIH in 2016, I began looking for a way to launch a study at the NIH Clinical Center that would allow us to better understand what’s happening in these situations and how to best address them. I was eventually able to connect with the Women’s Malignancies Branch at NCI, and the study launched in December 2019.
What are the study’s primary goals?
Bianchi: The main goal is to gather enough evidence to make professional recommendations about what to do when patients receive false-positive or “nonreportable” test results from prenatal screening, because there are big gaps in practice.
In this situation, some providers just say, “You’re healthy, you’re young, you’re pregnant. This is nothing.” Or they may only do a partial workup [of the pregnant person]. Or sometimes they refer the patient to an oncologist, who isn’t sure about how to proceed because there’s no standard for how to manage these patients yet.
The idea is to develop the evidence for a specific, prospective workup to determine whether the person has a malignancy and needs cancer management right away, even while they are pregnant. There’s also a part of the study that will help us better understand the patient’s experience in these situations.
Can you talk more about that?
Turriff: We’re trying to understand how people experience receiving these results and make decisions about whether to be screened for cancer during pregnancy.
Doctors and others involved in pregnancy care are concerned about causing anxiety in a pregnant person as a potential reason not to disclose the results, especially since it’s really beyond the scope of the prenatal screening test. But the perspectives of pregnant people who have received these results have not been studied.
So, we ask participants in our study to take part in interviews that explore their experiences receiving prenatal screening results that suggest the mother may have cancer, their decisions to be evaluated for cancer, and their thoughts on the risks and benefits of disclosing these results during pregnancy. We also collect surveys from study participants once a year so we can understand more about the personal impact of receiving these results.
Bianchi: We found that some of the participants have, for a variety of reasons, waited months before following up on their test results with an evaluation. However, as more clinicians become aware of this study, the interval is getting shorter. But there are some people who unfortunately have had really long delays.
What barriers have prevented people from joining the study? For instance, if people don’t have symptoms of cancer, do they prefer not to undergo more tests?
Turriff: About half of the people who are referred to the study choose not to join it. I think in most cases, they have no reason to suspect that they have cancer, so they do not see a reason to be evaluated.

Amy Turriff, Sc.M., National Human Genome Research Institute
All our participants are asymptomatic. They’re young. It’s hard for people in this situation to imagine that they could have something as potentially serious as cancer when they feel well. It’s also not uncommon for pregnant people to be reassured by their providers that it is unlikely that they have cancer. We see this impacting whether people choose to be evaluated and how quickly they follow up.
So far, what percentage of people in the study have been found to have cancer?
Bianchi: We’ve confirmed cancer in about 60% of the participants so far. The study workup includes coming to the NIH Clinical Center, having a full physical exam, blood work, repeated cfDNA sequencing, and then a whole-body MRI. Participants then meet with Dr. Annunziata and her staff to discuss the results of these tests and, if cancer is found, discuss the next steps for managing it.
What types of cancer are you finding?
Turriff: Going into the study evaluation, there’s a chance that any type of cancer could be detected. Lymphomas tend to be the most common type of cancer, but we’ve also seen some incredibly rare tumors in the study.
The interview data we have suggest that people expect that if they’re going to be diagnosed with cancer, it’s going to be at an early stage and highly treatable because they have no symptoms. And sadly, that’s not always the case. We’ve diagnosed people who seem entirely asymptomatic, and they actually have advanced metastatic cancer.
How is the study going, and how much longer will it go on?
Bianchi: We’ve enrolled about 70 participants and the study was planned to enroll 150, so we’re not closing enrollment anytime soon. There are already highly significant findings, and I think one of the take-home messages will be that with these prenatal tests, we have a genomic sequencing platform that was not designed to detect cancer, but it does.

Diana Bianchi, M.D., director, Eunice Kennedy Shriver National Institute of Child Health and Human Development
So, it does make you think about how it fits in with the liquid biopsy platforms being studied in cancer. These prenatal tests essentially are a liquid biopsy that, for certain types of tumors, work quite well.
How do you hope the findings from this study will impact care?
Bianchi: The big thing is that this study could provide the evidence needed to change medical management for pregnant people. And that would lead to insurance paying for the follow-up care of a pregnant person after they have an abnormal result.
That’s one of the reasons we originally wanted to do the study. Currently, very few insurance plans will pay for the workup following prenatal test results because there is not yet an evidence base to justify it. We don’t want people to be denied the workup because they can’t afford it.
The hope is that we can detect malignancies as early as possible. Also, despite the abnormal test results, not everyone in the study has turned out to have cancer. We have detected other conditions, such as fibroids, that can also release unusual DNA fragments into the blood.
We also want patients and providers to know that a pregnant person can safely undergo cancer treatment, particularly during the late second trimester to third trimester when the workup would be complete. The goal is to start treatment as soon as possible and not wait another 4 or 5 months until after delivery.






")

{kind=link}